

Sign up for our newsletter
GET INVOLVED
CONNECT WITH US
Phone number: +1 508-263-0112
MAILING ADDRESS: 45 Prospect Street, Cambridge, MA, 02139
© 2025 Sahiyo. All rights reserved | Terms & Conditions and Privacy Policy

Since 2014, Shared Nation has provided an online platform for citizens all around the world to come together in order to solve shared global problems like poverty, climate change, and refugee crises. Shared Nation embraces the lessons of history, which has shown that when people act towards shared goals, they can achieve extraordinary things.
This month, nominated by Gina Li, Sahiyo will be one of the projects participating in the August 2018 contest to be voted on to receive the digital community’s combined funds. Each month, general voting takes place for the first three weeks of the month, and in the final week of the month, a winner is selected from eight quarter-finalists.
What’s great about Shared Nation is that every participating project will be offered a small percentage of the pooled Shared Nation funds for taking part, but one lucky organization receives the vast majority of the funds.
If you would like to help Sahiyo become the August 2018 Winner, sign up for Shared Nation and vote today!
To sign up for Shared Nation and Vote for Sahiyo, click here. If you can’t pay that $2 fee, they will provide a free sponsorship for you.
You can also “favorite” Sahiyo and increase its ranking and visibility!

On July 10, judges of the Supreme Court of India observed that the “bodily integrity of a woman” cannot be violated while hearing a petition about Female Genital Cutting. The Court made this observation while hearing the arguments of a petition filed by the Dawoodi Bohra Women’s Association for Religious Freedom, which claims that FGC, as practiced by the Bohra community, is not “FGM” but “circumcision”, and is an essential religious practice that they have the constitutional right to follow.
In response to these arguments, made by DBWRF’s lawyer, Abhishek Singhvi, Justice Chandrachud said, “Why should the bodily integrity of a woman be subject to some external authority? One’s genitals is (sic) an extremely private affair.” The judges also observed that the practice cannot be imposed on those who do not want it.
This is not the final verdict of the Court, and the hearings in the case on FGC in India will continue.
Meanwhile….
On June 27, India’s Ministry for Women and Child Development denied the prevalence of Female Genital Cutting in the country – it’s second U-turn on the issue in the past 13 months. This denial came after a perception poll by Thomson Reuters Foundation ranked India as the most dangerous country in the world for women, based on a variety of parameters that included the practice of FGC. The Indian government responded to this poll by issuing a press release refuting and dismissing its methodology. In the press release, the Government also stated that “Female Genital Mutilation” is “not practiced in India”.
This is clearly at odds with the stand that the Central Government took in the Supreme Court just two months ago when it stated that FGC is “already an offence” under Indian law and asked the Court for guidelines on how to tackle the challenge of FGC.
This is not the first time that the government has made contradictory statements about FGC. Women and Child Development Minister Maneka Gandhi had first publicly acknowledged the practice of FGC in India, and the need to ban it, in May 2017. In December 2017, however, the Government dismissed the testimonies of several women who have spoken out about their FGC experiences by claiming, in the Supreme Court, that there is no “official data” to support the existence of FGC in India.
Such flip-flops leave FGC survivors in the lurch, unsure of whether their government is likely to support the end of a practice that continues to harm so many women and girls in India.
Read more:
Sahiyo comment – An appeal to Maneka Gandhi: Stop the flip-flops on Female Genital Cutting
Sign Sahiyo’s petition asking the United Nations for more investment towards research and advocacy on Female Genital Cutting in Asia.
Today, FGM/C is banned under federal law, yet, only 26 states in the U.S. have laws against it. Massachusetts is not one of them. According to the Center for Disease Control and Prevention, it is estimated that over half a million girls and women in the United States are at risk. Massachusetts ranks 12th in the nation for at-risk populations with an estimated 14,591 women and girls. Since 2012, the Massachusetts Women’s Bar Association has tried to advocate over and over again for a state law criminalizing FGM/C. Yet, to this day, no law has been put into place. The current bills, S.788, and H.2333 have been sent to a committee for study and most likely will not move forward either.
In an effort to raise more awareness on the issue and to prompt community action to encourage Massachusetts state legislature to pass such a law, Mariya Taher (a survivor of FGM/C) and Hanna Stern (an advocate against FGM/C), started a change.org petition calling on Governor Charlie Baker, Speaker of the House Robert DeLeo, and President of the Senate Harriette Chandler, to take action and protect all girls in Massachusetts, as FGM/C is nearly always carried out on minors, is a violation of the rights of children, and reflects deep-rooted inequality between the sexes that constitutes an extreme form of discrimination against women.
Massachusetts needs a bill that unequivocally reiterates that female genital mutilation/cutting is a form of violence. There are laws against domestic violence and sexual assault. We need a law against FGM/C as well.
Read more:
Learn which U.S. states have FGM/C laws.
By Priya Ahluwalia
Priya is a 22-year-old clinical psychology student at Tata Institute of Social Sciences – Mumbai. She is passionate about mental health, photography and writing. She is currently conducting a research on the individual experience of Khatna and its effects. Read her other articles in this series – Khatna Research in Mumbai.
Khatna, by virtue of being related to female anatomy, is often categorized as a women’s issue. However, one must also remember that it is a practice performed on uninformed and unconsenting children. We must move beyond defining it as a child or a woman being violated and look at it as a human being who is being wronged, and therefore the most comprehensive way to describe it would be a human rights violation.
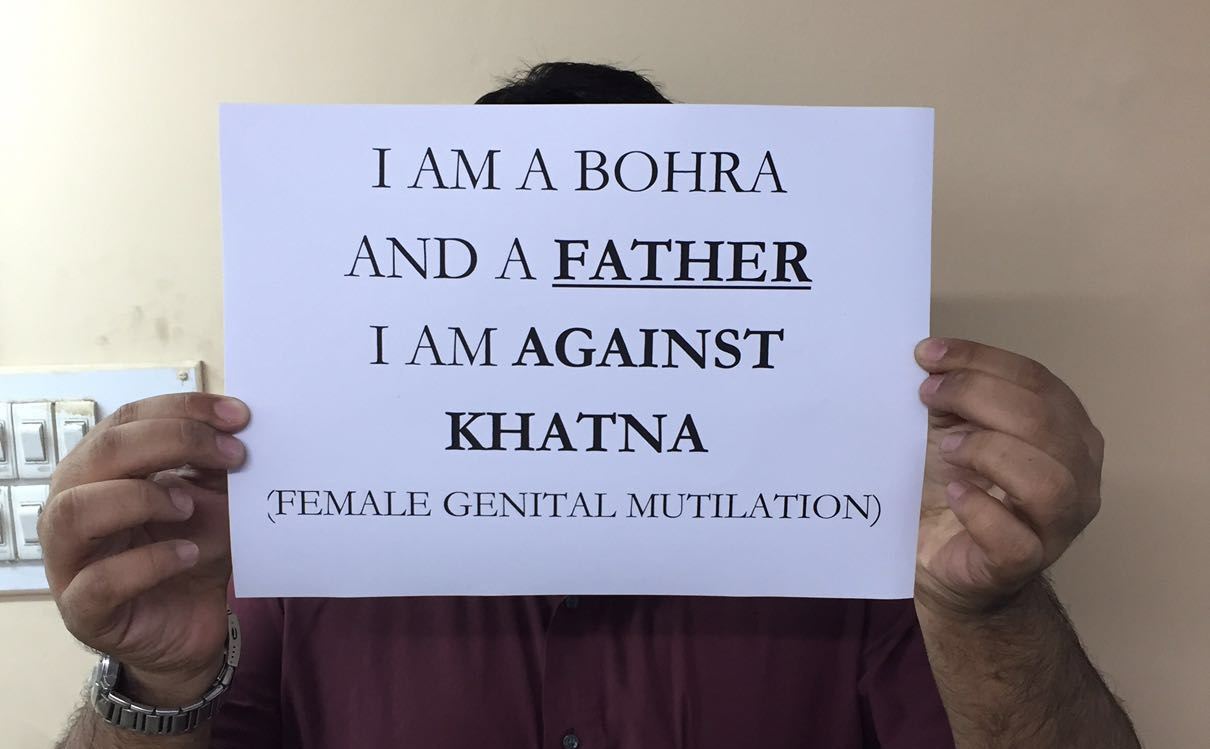
Despite it being a human rights issue, it appears as if not many people are willing to speak up against it, even though all people, especially men, need to do so. Within the structure of the Indian patriarchy, men enjoy power not only by virtue of their gender but also by their sheer number in our country. Therefore men can use their position of power to effectively tilt the weights in favor of women who are speaking against Khatna.
Although, ideally we expect all men to support us in the endeavour to end Khatna, we should also attempt to understand their hesitancy. Within the Indian patriarchal family structure, the woman is seen as the mistress of the house, in charge of children, while men are seen as masters for all things outside the domain of the house. Therefore any attempt by men to venture into the discussion concerning women’s bodies is seen as ill-mannered and a gross violation of clearly demarcated gender roles.
During my research, I met a father who became aware of Khatna and its consequences because he had daughters and therefore vehemently opposed it. He narrated the daily struggle of convincing his own mother against this practice. However, like many other men before and many after him, he was unsuccessful in dissuading the women in his family from continuing it on his daughter. He was blindsided by his mother and given the blanket argument that she knows better for a woman by virtue of herself being a woman.
Yet research has shown that with increasing education on khatna, more men are willing to campaign against it. Still, the onus of initiating a conversation on khatna among others lies with the women. Communication between men and women, especially husband and wife, is crucial for the discontinuation of Khatna. A woman I interviewed who had undergone Khatna took this initiative and began a conversation with her husband, which gave her immense strength and helped her protect their daughter from falling into the clutches of tradition. Research too corroborates the same: if more men are are part of the decision making process, the less the likelihood that Khatna would be performed on the girl.
The research linked above shows that men who wish to speak up are held back by their limited knowledge on the effects of Khatna.They are unaware of what is removed and what its ramifications are. The primary reason for this ignorance is the lack of conversations about women and their health among family members. This hesitancy to talk about women in front of men comes from the idea that women are equivalent to the family’s honour, therefore talking about aspects of their sexuality may be seen as a violation, thereby a disgrace, to the family’s honour. However, we must move beyond the archaic concept and understand that creating awareness about the ill effects that Khatna has on a woman’s body in no way defiles a family’s honour. After all, what honour can reside in pain?
Conversations about Khatna must begin, questions must be asked and collaborative measures between men women must be taken to put an end to this practice. There are several ways to oppose this practice. You may choose to speak out or you may to choose to silently protest; however, if active measures are not taken to resist it, then there is passive consent for the continuation of khatna, and we must understand that every time such consent is given, it means another child is being harmed. Therefore, let us come together for the children and do whatever we can, wherever we can.
To participate in Priya’s research, contact her on This email address is being protected from spambots. You need JavaScript enabled to view it.
Phone number: +1 508-263-0112
MAILING ADDRESS: 45 Prospect Street, Cambridge, MA, 02139
© 2025 Sahiyo. All rights reserved | Terms & Conditions and Privacy Policy